Ophthalmic Complications
Retinopathy
In diabetes, pathologic changes in the retinal vasculature pose a major long-term threat to vision. Retinopathy risk factors include poor blood glucose control, hypertension, smoking, nephropathy, dyslipidemia, diabetes duration, and type of diabetes (it is more common in type 1 than in type 2).
In nonproliferative diabetic retinopathy, microaneurysms, small “dot and blot” hemorrhages, hard exudates (lipid material that can be toxic to the retina), and retinal infarcts known as “cotton wool spots” appear. These changes tend to concentrate in the macula, where they can distort central vision.
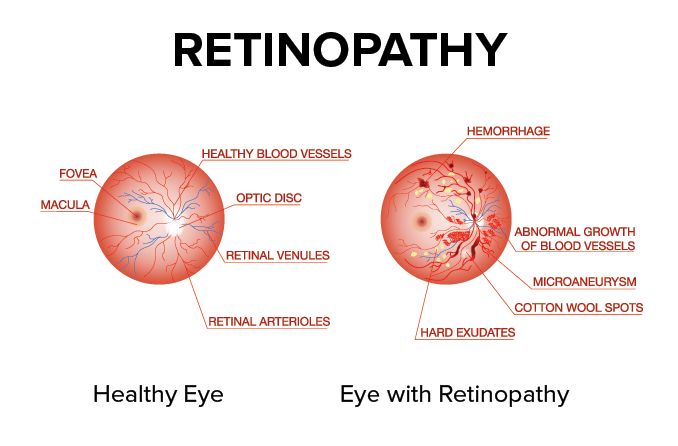
In proliferative retinopathy (neovascularization), fragile, abnormal vessels grow into the vitreous, presumably in response to ischemia. Vitreous hemorrhages cause symptoms ranging from “floaters” to complete visual loss. Ultimately, tractional retinal detachment can result. Retinopathy is not painful, so the condition can progress undetected by the patient.
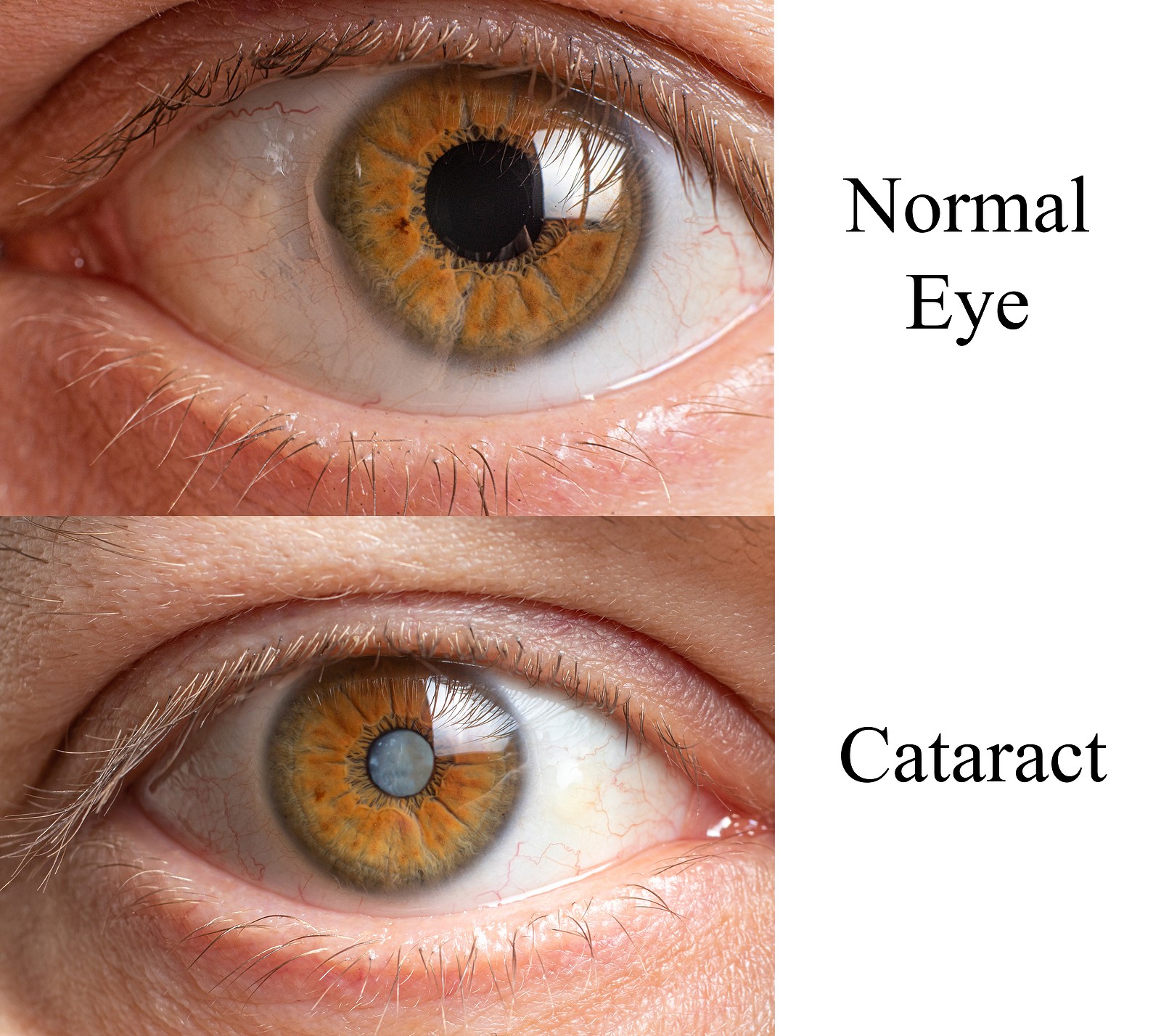
Glaucoma and Cataracts
Glaucoma and cataracts may develop earlier in diabetes patients, compared with those without diabetes.
Diagnosis
Retinopathy can be diagnosed by ophthalmoscopy with dilated pupils. Use of a fundus lens at the slit lamp allows a stereoscopic view and facilitates diagnosis of macular edema.
In fluorescein angiography, an intravenous injection of fluorescein followed by serial photography of the fundus can reveal leakage from microaneurysms, nonperfusion, and other useful information to guide therapy.
Treatment
Good control of blood glucose and blood pressure can reduce the risk of ophthalmic involvement and slow its progression.
For proliferative retinopathy where vitreous hemorrhage appears likely, panretinal laser photocoagulation often stabilizes neovascularization or even causes it to regress.
When diabetic retinopathy causes clinically significant macular edema (defined by severity of leakage and proximity to the central macula), photocoagulation can slow progression.
Individual microaneurysms can be obliterated, or a broader grid photocoagulated if the leakage pattern is diffuse. Intravitreal steroids and vascular endothelial growth factor inhibitors may also play a role in treatment.
Individuals with type 2 diabetes should have a dilated eye examination soon after diagnosis, and those with type 1 diabetes should be examined within 5 years of diagnosis. If eye examinations are normal and the patient is in good glycemic control, examinations every 2 years may be considered.
Although physical activity is a fundamental part of diabetes control, individuals with diabetes should be advised to favor aerobic exercise, which lowers intraocular pressure, rather than weightlifting, which has the opposite effect.
Nutritional Considerations
Evidence indicates that control of blood glucose, blood pressure, and blood cholesterol reduces the onset and progression of diabetic retinopathy. A specific diet therapy suitable for prevention of retinopathy has not yet been established. However, evidence from the Diabetes Complications and Control Trial (DCCT) associated diets high in fat and low in fiber with progression of retinopathy, suggesting that low-fat, high-fiber diets may have promise for reducing retinopathy risk. In addition, AGEs have been associated with the presence and progression of diabetic retinopathy, and low AGE diets have been shown to improve microvascular function when compared with high AGE diets in individuals with diabetes.
High vitamin A and C intake is associated with a reduction in open-angle glaucoma risk. In addition to lower CRP, HbA1C, and glucose, participants with diabetes who consumed more fruits and vegetables from the NHANES 2003-2007 had a 30% reduced risk of having diabetic retinopathy than participants consuming the least amount of fruits and vegetables.
No controlled clinical trials using nutrition therapies indicate that diet changes reduce cataract risk among individuals with diabetes. In the general population, however, a number of dietary factors are associated with lower cataract risk, including maintenance of ideal weight and normal lipid levels, high intake of antioxidant-containing foods, avoidance of alcohol, and avoidance of sources of galactose (i.e., dairy products).
